Published :
Updated :
 For all latest news, follow The Financial Express Google News channel.
For all latest news, follow The Financial Express Google News channel.
Across most healthcare economies, emergency departments (EDs), emergency rooms (ERs) and other emergency units are thought to be losing concerns for a healthcare facility, predominantly for high fixed costs required to ensure the delivery of daily 24-hour service. Up to 50 per cent of these costs are required for workforce remuneration with another sizeable chunk used up on expendables, laboratory diagnostics and radio-imaging services. A tertiary facility can expect to see 6.0 to 8.0 percent of its total budget going in to providing emergency-care services.
Established healthcare systems can expect to see an average profit margin of 8.0 per cent in both public and private sectors, but can this be expected in Bangladesh where emergency- care infrastructures do not exist and most of the economy is run out-of-pocket expenses? Established systems depend upon health insurance and national subsidies to recoup the costs of running an emergency unit. Compared to this, emergency care in Bangladesh wouldn't make sense. The closest data for comparison would be from India, where it is estimated that the average cost for each patient is USD 25 and the cost to run a fully fledged ED is USD 375 per hour. It would thus require the department to see at least 15 patients an hour to be cost-neutral.
Given the figures above, it would be daunting for any hospital administration to set upon the task of establishing an ED in Bangladesh. This is on the background that ERs in Bangladesh currently see only between 50 and 70 patients a month on average and the mean length of stay for patients is usually less than 15 minutes. The extraordinarily brief length of stay in the ER is down to the fact that minimal treatment activities currently occur in an emergency unit and most patients are immediately admitted to various in-patient areas, if any treatment is needed. At most, minor injuries are currently treated in the ERs of Bangladesh. With such statistics, it is obvious that standardising emergency services would cause a hospital to haemorrhage its revenue.
Or would it? A case example of the 250-bed Sadar Hospital in Cox's Bazar can provide some excellent insight into how improving the ED can actually bring in revenue for a health facility. Prior to the influx of the forcibly displaced migrants from Myanmar in late 2017, the ED was typical of any district hospital. Despite a departmental floor-plan layout, emergency care was delivered from only one room in the method described above. However, the extra burden of over 1,000,000 refugees in the tertiary hospital's catchment area meant that services had to be improved for efficiency, and the International Committee of the Red Cross (ICRC) took on this task in 2019. Within two years, the number of patients jumped from 20,000 annually to over 100,000. Currently, the department often sees up to 500 patients a day.
Much of this success can be credited to a change in culture within the department that eventually translated to a change in culture across the community in regards to its Emergency Department. As patients came to expect more from their emergency department, they developed a trust in its service, which enabled the healthcare professionals to see, treat, and discharge appropriate patients straight from the department, without the need of inpatient admission. This change in culture reduced not only the burden on the inpatient services of the hospital but also on the overcrowding by emergency patients and their numerous attendants.
As stated at the outset, some of the highest costs in the ED are from laboratory diagnostics and radio-imaging services. As is true for most of the health systems in Bangladesh, this is where most EDs can earn their revenue. However, having such investigations done in a standardised emergency department does benefit the patients by having the number of unnecessary tests trimmed down.
It would now be logical to think that standardising emergency care and setting up EDs across Bangladesh would boost hospital revenue considerably. This is true to a point. An indefinite increase in patient numbers across the finite footprint of an emergency department unfortunately leads to stress and errors. Such stress manifests both in patients (due to extended waiting time) and staff (due to disproportionate staff-to-patient ratios). Errors in the emergency department, no matter how seemingly insignificant, can have morbid consequences given the nature of care provided.
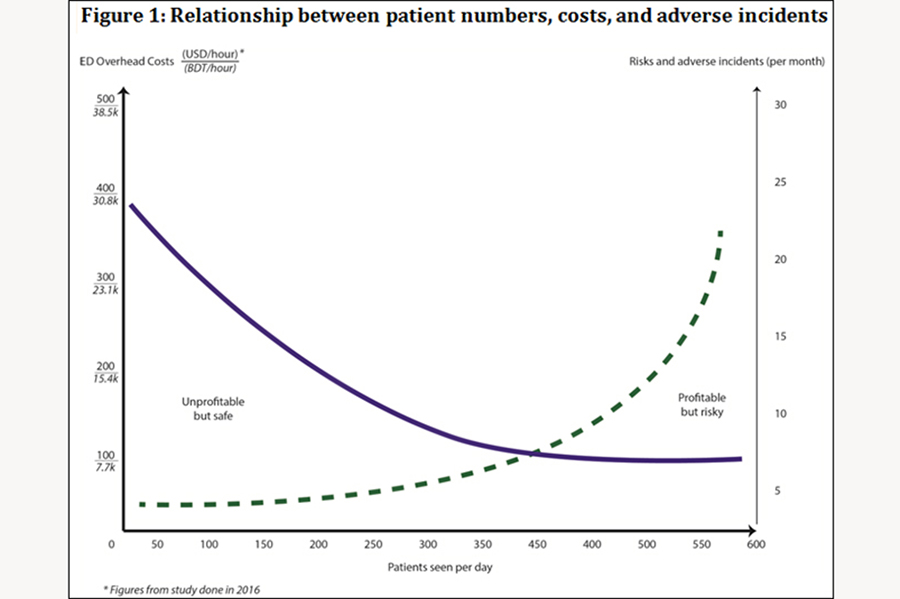
The graph in Figure 1 below shows the relationship among these three factors.
Overhead costs are the most when the minimum number of patients is seen. In line with the Law of Demand, as patient numbers increase, the overhead costs decrease to a base level (solid curve against the primary axis). However, once the department starts to get overcrowded, the risks in the department and the adverse incidents start to increase (dotted curve against the secondary axis). There is no doubt that the safety of the patient is paramount, but it is also crucial that this high level of care remains sustainable.
It is, therefore, vital for the hospital administration to assess the appropriate resources required in the emergency department for the size of their defined catchment area. In doing so, it may very well be that ED cannot see the numbers required to keep costs at an optimal level. In addition, there are always cases that require emergency care without the possibility of remuneration. The health economy of Bangladesh is surprisingly well- equipped to deal with such situations.
As Bangladesh moves from a low-income to a middle-income economy, the presence of corporate institutions is increasing. These institutions have it built into their governance to help improve their community by means of their corporate social responsibility (CSR) funds. Many hospitals in Bangladesh are part of a larger business venture and can, therefore, easily tap into CSR funds from their parent company for upgrading emergency care. If not, corporate organisations can be directly approached for disbursement. Another avenue in Muslim- predominant Bangladesh is to access zakat funds from charitable organisations and internal staff to pay for the healthcare of those burdened with poverty.
The bottom line is that all healthcare facilities in Bangladesh should be prepared to manage emergency-care presentations appropriately (for their size and location) because in doing so, they will not only improve their organisational capabilities but also many of the national health goals that Bangladesh has targeted.
Dr Mir Saaduddin Ahmad is a specialist in international emergency medical care working with the ZABS Foundation in Bangladesh and Doctors Worldwide in the UK. He is also a consultant in emergency medicine in the NHS, based in London. dr.msahmad@gmail.com